
Future in Our Hands Womens Co-operative, Oku
Future In Our Hands Cooperative Oku
 FIOH Oku is a women’s farming cooperative made of over 5 Common Initiative Groups (CIGs) representing over five villages in Oku Subdivision. It was created on the 22nd of September 1999. It encourages the spirit of hard work, cooperation and togetherness in women. It is called a women’s cooperative because 95% of members are women. Her creation was thanks to the interest SHUMAS NGO and Future Our Hands had to empower women and the vulnerable in the Oku community. It has as motto: educate a man, educate an individual; educate a woman to educate a whole nation. This is because of the socio-economic importance of a woman in the purely African village community like Oku. Some of the projects realised by FIOH-Oku:-
FIOH Oku is a women’s farming cooperative made of over 5 Common Initiative Groups (CIGs) representing over five villages in Oku Subdivision. It was created on the 22nd of September 1999. It encourages the spirit of hard work, cooperation and togetherness in women. It is called a women’s cooperative because 95% of members are women. Her creation was thanks to the interest SHUMAS NGO and Future Our Hands had to empower women and the vulnerable in the Oku community. It has as motto: educate a man, educate an individual; educate a woman to educate a whole nation. This is because of the socio-economic importance of a woman in the purely African village community like Oku. Some of the projects realised by FIOH-Oku:-
- Improving the processing and transformation of corn and cassava through mills and haulers donated by SHUMAS and her partners.
- Offering loans to members at very minimal interest rates through a scheme developed by SHUMAS.
- Through SHUMAS there has been the development of community health infrastructure for the village of Lui.
- Regular production of organic food crops and other natural products for income generation and food security.
- Attending agro-pastoral shows to market their produce.
- Training and practising sustainable and integrated farming and livestock productions methods amongst her members.
- Training and application of agroforestry techniques to her membership.
Oku is located in Bui Division of the North West Region of Cameroon. It is made up of 36 village communities mostly living along the slopes of the Kilum Mountain. The people depend mostly on forest resources, subsistence agriculture, cash crop farming, livestock production and local artisan work for their livelihood. The Kilum Ijim Forest found in the community is a naturally preserved moist montane forest with a surface area of about 20,000 hectares. It is located in the Mount Oku Ridge in the Bamenda Highlands and forms part of the High Plateaus Agro-ecological Zone of Cameroon. The geographic location of the area is latitude 6°07’N – 6°17’N and longitude 10°20’E – 10°25’E. It has very important and threatened Afro-Montane endemic animal and plant species such as Prunus africana amongst others. It is an internationally important biodiversity hotspot and a critical zone for carbon sequestration within the High Plateaus Agro-ecological Zone.
The Kilum area is one of the highly populated locations in Africa and Cameroon in particular, accommodating 144,800 people occupying about 328 km2 (439.3persons/km2); hence, high pressure on resources is inevitable. There has been progressive deforestation and degradation mainly due to agricultural expansion, forest fire and overgrazing. Fuel wood harvesting has also been a major cause of deforestation and forest degradation. The late 1980s decline in coffee prices triggered many farmers to migrate further up the slopes in search of new land to increase income through alternative crops.
Within two years of its formation the activities of the co-operative had a profound positive impact on the lives of the women:
Former situation
- We were scattered and never cared to come together because we did farming far away from our homes because of the eucalyptus trees that were planted around our homes by men.
- We thought that only men had the right to inherit the property of parents. We never attended seminars and training programmes.
- We were shy to express ourselves among men and only played the part of listening.
- Our opportunities for income-generation were very limited.
- We thought HIV/AIDS was a curse from God and an opportunity for white people to sell us condoms.
- We thought that bread and cakes production was the duty of men. We did not know the importance of business – buyam sellam.
- If a woman was illiterate when she married we thought this was the last chance for her to become literate.
- Single parents had to resort to work on farms just to feed the family. They had insufficient income for their children’s education.
- Women believed that only men had the right to determine how many children they should bear.
- Husbands decided which political party their wives should vote for in Elections.
- Only men had the right to erect buildings and got the credit for doing so despite the help of women.
- Men brought in second wives without the consent of the first wife, claiming it is their right.
- Women thought only of their own needs and rarely discussed problems together. We did not engage with women from other villages.
- Widows used to sleep on bare floors in very smokey houses that constituted a breeding ground for germs and diseases.
Current situation
- We now farm around our homes and have enough time to come together. Children now attend school as they do not have to come with us to distant farms. We have gained experience by coming together e.g. joined savings and credit groups with small interest charged on loans. We now have small businesses that help to solve some of our problems like paying for school fees and drugs. We are healthy and do not have to rely on our husbands for money.
- We have attended many seminars organised by SHUMAS and the Diocesan Commission for Justice and Peace, Bishops House, Kumbo, Human Rights agent and the International Federation of Female Lawyers in Cameroon.
- Now we express ourselves freely because of the lectures from SHUMAS and human rights agent who told us that every person is the same before the law and has the right to express his/her views freely.
- We now produce tablet and powder soap and hire a hand cart for transporting items.
- Through seminars we have learned that HIV/AIDS is real. We go out to schools and talk on the rural radio about the dangers and the precautioins that must be taken. There have been significant changes in sexual behaviour as a result.
- We now have our own small bakery and members can take part in bread making and poff poff production. We sell what we make and employ male youths to carry to far distant places by motorbike to sell.
- The eucalyptus replacement project has enabled women to have more time to engage in adult literacy classes. These include married women who were once illiterate.
- FIOH Oku has encouraged single parents to join the co-opertive and learn how to engage in income generating activities. The co-operative has provided them with small loans and they are now able to sell items in the market. Some have been able to send their children to school and have given testimonies on how their lives have improved.
- From the lectures and seminars women became more aware that men and women should jointly agree the number of children they should bear.
- Through the education of the human rights agent and messages from Mike Thomas of the FIOH UK Fund, women now know their rights to vote in their own right.
- Women now realise that they can take the initiative in putting up a building. Our women have bought a plot of land and have erected their own meeting hall.
- Through the co-operative we have taught women the importance of marriage certificates and various types of marriage . If monogamy is the choice then men have no right to bring in a second wife or mistress.
- We now have exchange visits with other womens co-operatives in our network. We exchange ideas and learn from each others experience.
- Now most women, especially FIOH women, do not now sleep in such houses. When their husbands die they sit in a special room with friends who comfort them.
![]()
Follow us on Facebook:
www.facebook.com/fiohfund
Follow us on Twitter:
twitter.com/fiohnet
Please share our links with your friends to help us reach a wider audience.
Ebola identification and prevention programme

Ebola programme
FIOH Sierra Leone carried out this programme in 2015. The FIOH Fund contributed £7,138 towards this project located in the Tonkolili, Bombali and Port Loko districts in the north of the country. Most of the funding came from Bread for the World.
Where does Ebola come from?
The first known incidents of the Ebola virus were in 1976. There were two simultaneous outbreaks in Nzara in Sudan and Yambuku in Zaire (now the Democratic Republic of Congo). The name of the Ebola river near Yambuku was given to the new epidemic.
Outbreaks have mainly occured in remote villages in Central and West Africa, close to tropical rainforests.
The main outbreaks were in West Africa, mainly in Guinea, Sierra Leone and Liberia.
Ebola is described by the World Health Organisation (WHO) as “one of the most virulent viral diseases known to humankind.”
There are five distinct species of Ebola and the survival rate ranges from 25 to 90%. There is no licensed vaccine for Ebola although several are currently being tested.
How is the Ebola virus transmitted?
- Ebola is passed to humans through close contact with the blood or bodily fluids of infected animals. Fruit bats, monkeys and chimpanzees can all carry the virus.
- Ebola then spreads through human-to-human transmission, again from contact with blood or bodily fluids.
- Burial ceremonies where mourners touch the body of the dead person can also spread the disease.
- The incubation period (the time from infection to the onset of symptoms) is between two to 21 days.
- People remain infectious as long as their blood and secretions contain the virus.
What are the symptoms?
Initial symptoms include the sudden onset of a high fever, muscle pain, general weakness, headache and sore throat.
Further symptoms include vomiting, diarrhoea, rashes, damage to the kidney and liver function.
In some cases symptoms can include both internal and external bleeding.
There is no known cure or vaccine for ebola.
How can the virus be prevented?
- Routinely cleaning and disinfecting farms to inactivate the virus.
- Animals should be handled with gloves and protective clothing. Meat should be thoroughly cooked before eating.
- If an outbreak is suspected in animals, the premises should be quarantined and infected animals culled.
- Avoiding physical contact with people infected with Ebola and protective clothing must be worn.
- Washing hands after visiting patients in hospital, or after taking care of those infected at home.
- Inform the authorities when a community is affected so containment measures can be taken.
- Ebola victims should be buried quickly and safely, with no direct contact with the corpse.
What is being done to treat it?
Several vaccines are being tested, but none have been approved for clinical use.
Severely ill patients require intensive supportive care. Patients are frequently dehydrated and require oral rehydration with solutions containing electrolytes or intravenous fluids.
Background to the project and problem analysis
 In May 2014 the Mano River Union countries (Sierra Leone, Liberia and Guinea) experienced an outbreak of ebola. Between May and October 2014 the disease left over 4000 people dead in this part of West Africa. In Sierra Leone the epidemic spread across the length and breadth of the country.
In May 2014 the Mano River Union countries (Sierra Leone, Liberia and Guinea) experienced an outbreak of ebola. Between May and October 2014 the disease left over 4000 people dead in this part of West Africa. In Sierra Leone the epidemic spread across the length and breadth of the country.
Since the outbreak the Future In Our Hands – Sierra Leone together with Youth with Focus, Kankalay Youth Development, Sorbeh Nyagah Women’s Association and God is God Ministries were part of the national Sensitization Team engaged in Community Education on the Prevention and spread of the Ebola Virus. Our messages focused on the causes, symptoms, preventive measures and required action in the case of infection. Although we were fairly satisfied that most communities were fully aware about the outbreak and the infectious nature of the disease, we realised the need to take the fight to another level as the spread of the disease was not then contained. We realised that the strategy then adopted was mainly focused on providing supportive treatment for infected patients at specially established treatment centres in Kenema and Kailahun; then scaled up to Freetown. Initially the follow-up of contacts was difficult due to mistrust and resistance of the local communities; attributing the infection to witchcraft, failing to take sick patients to hospitals and resisting attempts to collect dead bodies by the authorized burial teams for sanitary burials. These challenges led to a failure to effectively interrupt the chain of infection. The situation was aggravated by the very weak capacity of local health facilities as they were not able to adequately mount a consistent response due to ill preparedness and loss of staff frightened by the high morbidity among their ranks. This utter state of paucity weakened the overall health system even further. Communities were not equipped to isolate suspected cases effectively. This led to an increase in stigma, discrimination and fear. This awareness among FIOH-SL ignited an action to build community capacity to respond to the ebola epidemic by forging stronger partnership and collaboration with state actors and non-state actors.
The death of many health care workers in the country created panic and mistrust in hospitals, with reports that some health care workers were abandoning their posts. Ebola is almost universally fatal. Victims were socially stigmatized and isolation represented an offense and family shame.
Some of those affected by the virus were either abandoned or rejected by their families during hospitalization. In the isolation ward in particular, the most harrowing experience for victims and health workers was the loss of friends and colleagues who died next to them. The reluctance of hospital personnel to treat them and the abandonment by medical staff including the refusal to admit visitors was also difficult to bear for most patients. The grief for family members who did not survive was also very intense. Some of those who survived either tried to escape from their families or immediate neighbourhoods for fear of stigmatization. Those who survived, even though completely healthy, were feared by others. People did not want to come near them or have anything to do with them. Even their children were told not to touch them and wives were told to go back to their home villages and communities. The discrimination extended to family members and friends, who were regularly shunned at market places and other public areas. For the community, the psychological trauma of losing loved ones and witnessing death on a large scale and ebola burial methods were very distressing and traumatic and often caused severe long term mental health consequences for the relatives of the victims.
Prior to the outbreak of the ebola virus in the country, Sierra Leoneans were much concerned about family members’ sicknesses, deaths and other social issues. In most cases the families even raised funds to bury their dead with the full participation of community members whether the community was heterogeneous or homogeneous. The community members also provided peer support for those with serious illnesses or for bereaved family members. But with the collapse of this unique practice due to the ebola virus outbreak in the country, there were very serious family divisions and animosities. For instance, family members could not touch their loved ones in the event of sickness or death, while members of the community.
The FIOH Sierra Leone forum saw the need to promote peace among families, in the communities and in the nation as a whole. The forum aimed to provide psychosocial support to survivors, family members and volunteers, including social workers and clinicians. Volunteers, mainly community leaders, social workers and family members, were trained to conduct community sessions/outreach campaigns for the mitigation and reduction of stigma and fear of ebola survivors and their families in the communities.
Objectives
Overall Objective:
- Eradicate Ebola Virus Disease (EVD) from communities by April, 2015
- Increased respect for human right of EVD infected person by April, 2015
Specific Objectives:
- Increased community awareness to prevent ebola
- Strengthened community health services able to prevent ebola transmission
- Increased protection of ebola susceptible person
- Improved environmental sanitation and personal hygiene
- Re-integrate affected communities
Coordinate and monitor project implementation.
Project activities
- Increased community awareness to prevent ebola
- Volunteers ans staff trained on ebola prevention and contact tracing
- House-to-house visits carried out to identify sick persons for referral to health facilities.
- Reports made to district Ebola Operation Center (EOC) of all suspect persons or death and samples collected for ebola test.
- Flash electronic thermometers distributed.
- Health workers trained in Universal precaution and use of PPE.
- Community volunteers trained to work with burial teams.
- Infected persons transported to holding centers.
- Relief items including blankets, food, and water distributed to holding centre.
- Dead bodies collected from communities for sanitary disposal.
- Family members trained on hand washing and waste disposal methods.
- Ebola confirmed premises disinfected.
- 30 hand pump water wells constructed.
- 30 hand pump water wells rehabilitated.
- 600 ventilated pit latrines constructed.
- Agricultural packages (seeds & tools) distributed to 100 farm family heads.
The table below summarises the situation in the three regions in mid 2015:




Protective measures. Training. Safe burials.
If you would like to support the work of the FIOH Fund please make a DONATION:
![]()
Follow us on Facebook:
www.facebook.com/fiohfund
Follow us on Twitter:
twitter.com/fiohnet
Please share our links with your friends to help us reach a wider audience.
Poverty alleviation in the Thar Desert
 Poverty Alleviation in the Thar Desert
Poverty Alleviation in the Thar Desert

For the people living in the Thar Desert region of Sindh, drought is a frequent threat and one of the major causes of poverty and deprivation.
This project (June 2004 – Nov 2008) involving the following activities helped 1,100 families (6,600 people) in 20 villages cope with this situation and build up resilience for the future:
- Village Development Organisations were
established in 10 villages. - Provision of 800 water harvesting tanks and 800 fuel efficient stoves.
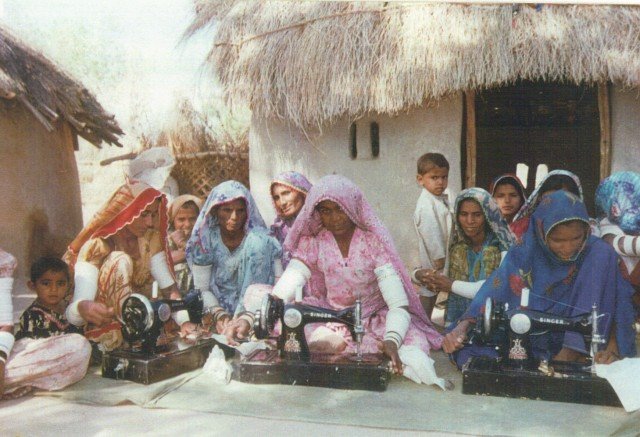
- Provision of materials and training of women in embroidery and their civil and political rights.
This video gives an indication of what life is like for people living in the region:

Training was also provided for the families and the community as a whole in HIV/AIDS awareness, controlled grazing practices and management techniques.
Water harvesting tank





The outcomes of the project included:
- A 12% increase in the numbers of girls being enrolled in primary education.
- A drop of 10% in the incidences of cholera and infant mortality.
- A 27% decrease in eye problems and chest infections of women beneficiaries.
- Better access to water by all the beneficiaries during periods of drought.
- Communities gaining more confidence to campaign for their statutory rights and the women becoming more involved in village decision making.
The project managing partner, Participatory Village Development Programme (PVDP), was well established before this project started.


The project was visited by FIOH Fund assessors, Eddie Thomas in 2005 and Joanna Heaven in 2008.
The PVDP poverty reduction model, which involved establishing Village Development Organisations and an Integrated Management Committee, was used in the Eucalyptus Replacement Project in Cameroon and proved to be a very effective method of involving all the stakeholders.
Poor people benefitting from the project:
Three case histories
If you would like to support the work of the FIOH Fund please make a DONATION:


Cyclone relief in Orissa
 Cyclone relief project – the green eye club
Cyclone relief project – the green eye club
This project was started after the severe cyclone that hit the coast of Orissa in 1999 to involve children in (i) growing tree seedlings and green vegetables to reduce vitamin A deficiency (the main cause of night blindness) and (ii) the identification of old people with eye cataracts.


A red mark on the side of the school in the coastal village of Kiada, Ersama Block, indicates the level at which the water settled on the 29th Oct 1999 after a 9m tidal wave generated by a severe cyclone caused devastation along the Orissa coastline.



Women, most of them widows as a result of the tidal wave, were provided with vegetable seeds to establish their own kitchen gardens.
Children started planting tree seedlings in March 2,000 and helped with a simple procedure to identify old people with cataracts.
If you would like to support the work of the FIOH Fund please make a DONATION:

Farm and tree planting nursery, Muniguda, Orissa
Background
In 1984 Eliazar Rose, whose parents once suffered from leprosy , established a Research Trust with some of his friends to help the the tribal people in the Rayagada District of Orissa suffering from leprosy, cholera, malaria TB and hepatitis. Although this early work was focused on these diseases, it was soon recognised that addressing the needs of the people required a more holistic approach that would increase incomes whilst at the same time preserving the natural environment on which the tribal people depended.
In 1985 an organisation named the New Hope Rural Leprosy Trust was established to develop this approach. The FIOH Fund has supported some of the smaller projects of New Hope since 1995. FIOH UK has also supported projects before the affiliated charity (FIOH Fund) was established.
Farm and tree planting nursery
 An 11 hectare plot of land was purchased by New Hope with a grant of £2,500 from the FIOH Fund in 1990. Part of the land was used to establish a nursery for 60,000 tree seedlings. These were later supplied to tribal people living in the surrounding hills where demand for fuelwood had been causing deforestation and erosion.
An 11 hectare plot of land was purchased by New Hope with a grant of £2,500 from the FIOH Fund in 1990. Part of the land was used to establish a nursery for 60,000 tree seedlings. These were later supplied to tribal people living in the surrounding hills where demand for fuelwood had been causing deforestation and erosion.
Bricks were also produced here from the local clay and fired using waste rice husks. Some of the bricks were used to construct on-site facilities for vocational training for both leprosy and polio patients.
If you would like to support the work of the FIOH Fund please make a DONATION:
![]()
Follow us on Facebook:
www.facebook.com/fiohfund
Follow us on Twitter:
twitter.com/fiohnet
Please share our links with your friends to help us reach a wider audience.